


Coils, Cuts, Condoms, and Chemical Contraception
Coils, Cuts, Condoms, and Chemical Contraception
10 min. read


Why oh why do we still depend on antique methods for contraception? The pharmaceutical industry invests billions of dollars to develop new drugs and devices using genetic engineering, cell cultures, robotics, artificial intelligence, and so on. So why are we stuck with condoms, coils, diaphragms, and other common stock? Even the acclaimed oral contraceptive pill has only gradually evolved in its sixty-year history. I explore some reasons below, but I have more to beef about first.
Why oh why oh why did a country that brags as the great defender of liberty impose on citizens’ freedom to choose to have children or none? Even dictating contraception in modern times, from reversible methods to permanent sterilization. Surely it is right that people make their own decisions except in extreme cases after due process of law. Legislatures and courts should not be trusted to rule what a man and a woman consent to do in their bedroom. Liberty cannot be unlimited, of course, unless you are Robinson Crusoe on Desert Island, but overweening interference in reproduction is shameful and not just a relic of the past.
If we pick an individual to blame, we might begin with Anthony Comstock, the Victorian purity crusader. Horrified by lewd behavior in New York City after leaving roots in rural Connecticut, he gathered a movement in 1873 to persuade the U.S. Congress to prohibit the mailing of advertisements and contraceptive devices across state lines. I had never heard of the Comstock Act until I read the newsfeed one day. It is still in the statute book and might be used to stop mail orders of contraceptives and mifepristone, a progesterone-blocker for first-trimester abortions, uterine fibroids, and Cushing’s adrenal syndrome. Comstock’s ghost still stalks the hallways of state capitols.
A few weeks ago the oldest Justice on the bench expressed an opinion that the U.S. Supreme Court “should reconsider” past rulings. I think he implied Griswald v. Connecticut. One of the bluest states, Connecticut upheld repressive fertility laws. Estelle Griswold in the Connecticut branch of Planned Parenthood and the Yale University fertility specialist Dr. C. Lee Buxton were indicted in 1965 for advising married couples about avoiding unwanted pregnancies. After being found guilty, the judge fined them but stopped short of custodial sentences of up to a year. The Supreme Court quashed the lower court ruling based on citizens’ rights under the Fourteenth Amendment as it also swayed Justices eight years later over Roe v. Wade. They concluded, “Connecticut’s birth control law unconstitutionally intrudes upon the right of marital privacy …”
Fifty years earlier, the redoubtable Margaret Sanger marched into the fertility battlefield promoting a right to birth control. It chimed with her social activism and standing in the women’s suffrage movement. The lifetime birth rate had fallen steadily from seven in 1800 to an average of three in 1916 with corresponding decreases in maternal deaths and infant mortality. Nevertheless, many poor women still struggled with larger families than they could cope with and lacked the means to limit their fertility. That year Sanger opened the first American clinic in New York City to offer birth control or family planning as we prefer to call it today. Most women came without their partner or his knowledge.
Persecuted by the authorities, she fled to England where she met a counterpart, Marie Stopes. On returning home, the police closure of her clinic resembled their subsequent raids on speakeasies that sold illegal liquor. A judge sent her to prison like a bootlegger, and not for the last time.
Besides humanitarian goals, she hoped more voluntary control over fertility would curb world population growth. Unfortunately, her reputation suffered later on from criticism of a neocolonial attitude to fertility control in India and sympathy for the then-popular and false science of eugenics. Nevertheless, she deserves credit not only for access to contraception but for accelerating the development of hormonal methods. She knew the reproductive endocrinologist Gregory Pincus, famous for in vitro fertilization in rabbits and other breakthroughs. He convinced her that progesterone treatment mimics the pregnancy block to ovulation, although financing a project would be hard in the political climate.
She introduced him to her friend and fellow suffragette Katherine McCormick. The heiress of a fortune from the inventor of the mechanical reaper funded most of his research, and with perfect timing. The major steroid hormones were revealed before World War II. Purified progesterone (and cortisone) became available afterward by extracting a precursor from Mexican yams, and another progestin, norethindrone, was synthesized to replace the natural hormone slowly absorbed from the gut. Pincus partnered with the Harvard gynecologist John Rock for the clinical phase of research. Combining synthetic estrogen with progestin to give greater control of the cycle created a pill 100% effective. Derivatives are now used by 150 million women worldwide. After Rock clandestinely trained his medical students in sex physiology the loyal Catholic doctor tried to persuade the Vatican to approve the Pill on the tenuous notion that it extends the safe days of the menstrual cycle. Pope Paul VI didn’t swallow it. His 1968 encyclical Humanae Vitae vitiated any morality from hormonal contraception. The rhythm method won his approval because it is “natural,” if you believe deliberate abstinence at the unsafe time of the cycle is ordained by nature. The Pill is a wonderful gift of science and even safer with a low estrogen content, although some women shouldn’t use it, and a third stop after a year or two. There never will be a perfect product for everyone but the search goes on, dreaming of zero conception plus zero harm, it draws down asymptotically toward the X-axis.
Pincus and Rock wanted to keep the monthly menses. But what we as modern people regard as natural is rare in hunter-gatherer societies, and was probably the same for prehistoric ancestors. In the first instance, intercurrent ovulation and conception (superfetation) are blocked in pregnancy. In the second, fertility is suspended by a neurohormonal reflex while infants depend wholly on breast milk, lasting 3-4 years in those societies. It was no leap of intuition to wonder if the Pill can be adapted to imitate years of amenorrhea before pausing for menstruation. Colleagues at the Medical Research Council Unit across the road from my office in Edinburgh launched a clinical trial in the late 1970s to test a “tricycle” pill. The women gave positive reports, even welcoming a three-month break from the tyranny of more regular periods. Edinburgh doctors have been at the forefront of reproductive health research since James Young Simpson introduced anesthesia for pain in childbirth, but this time they were scooped out of a reward.
I didn’t hear more about the experimental regimen until I moved to the Eastern Virginia Medical School to replace the retiring endocrinologist, Gary Hodgen. I then learned about his patent for a tricycle pill with a smart name, Seasonale. It had almost reached the F.D.A. for approving it for the fertility market. Roger Short, the former director of the MRC Unit, expressed rage at hearing his invention had been pocketed. I hoped he didn’t blame me. Novelty is a primary criterion for patent eligibility, but the U.S. Patent Office erred by approving an invention already published by others.
The Pill is not the only hormonal contraceptive, of course. A synthetic progestin in the morning-after pill (Plan B) is an ovulation blocker and its other effects help to make it highly effective.
GNRH is a hypothalamic hormone that the Edinburgh unit invested time in research. The non-steroidal molecule drips from nerve endings to travel a short distance to the pituitary gland to stimulate the gonadotrophic hormones, LH and FSH. Synthetic analogs of GNRH or vaccines have similar effects to damaging the pituitary stalk from, say, a whiplash injury. The paired hormones shut down and so, in consequence, does ovarian function. The prospects for contraception are spoilt by hormone replacement to counter a drastic reduction in estrogen. However, they are useful for the humane control of feral animals or wildlife pests, and even elephants by shooting immunocontraceptive darts.
Since vaccination protects us from measles for life and tetanus for ten years, why isn’t a contraceptive vaccine available for humans? The W.H.O. supported a program to neutralize the pregnancy hormone HCG until withdrawing it close to the finishing line. Being a self-protein, HCG had to be coupled to the tetanus toxin to fool the immune system into attacking the hormone as an alien. Volunteers treated with the vaccine continued their menstrual cycles as before but as antibody titers declined the risk of breakthrough pregnancies and miscarriages increased. A promising program snuffed out from variable responses to treatment and the need for booster injections.
Men should have a larger role in family planning than a footnote (ideally equal). Whereas women choose from pills, patches, implants, and shots for hormonal contraception, men have none of those options. When I asked a friend in the pharmaceutical industry he told me his company looked at the prospects and turned away.
It is not for lack of trying or our ignorance of spermatogenesis. Pills have been formulated to work in men by analogy with women. When a progestin is taken to stop the production of sperm and the male hormone, the pill must be combined with a synthetic form of testosterone to avoid castration-like effects. It clears sperm from the semen, although relatively slowly, which is to be expected considering the millions of sperm compared to one ovulated egg. Surveys of Scottish men have revealed support for a hormonal pill, implant, or even a gel in the latest studies, but complained in clinical trials about the side effects of mood changes and ebbing libidos. Condoms are still in business, only evolving from butcher’s animal bladders and intestines for Medieval men and linen tubes for Ancient Romans to latex today.
If a man wants to permanently avoid impregnating his partner, he has an excellent option. I had a vasectomy after the birth of my second child. A 15-minute procedure under local anesthetic is no sacrifice compared to tubal ligation in women. I never had cause to worry, nor was I ever aware of it unless I went “down there” for an inspection. Two small knots are not the remnants of ligatures. They are where sperm burst out of their tubes to form granulomas in local autoimmune responses. The immune system was never introduced to sperm when it learned to distinguish self from non-self tissues before birth, so when they formed at puberty they are kept hidden from surveillance inside a blood-testis barrier.
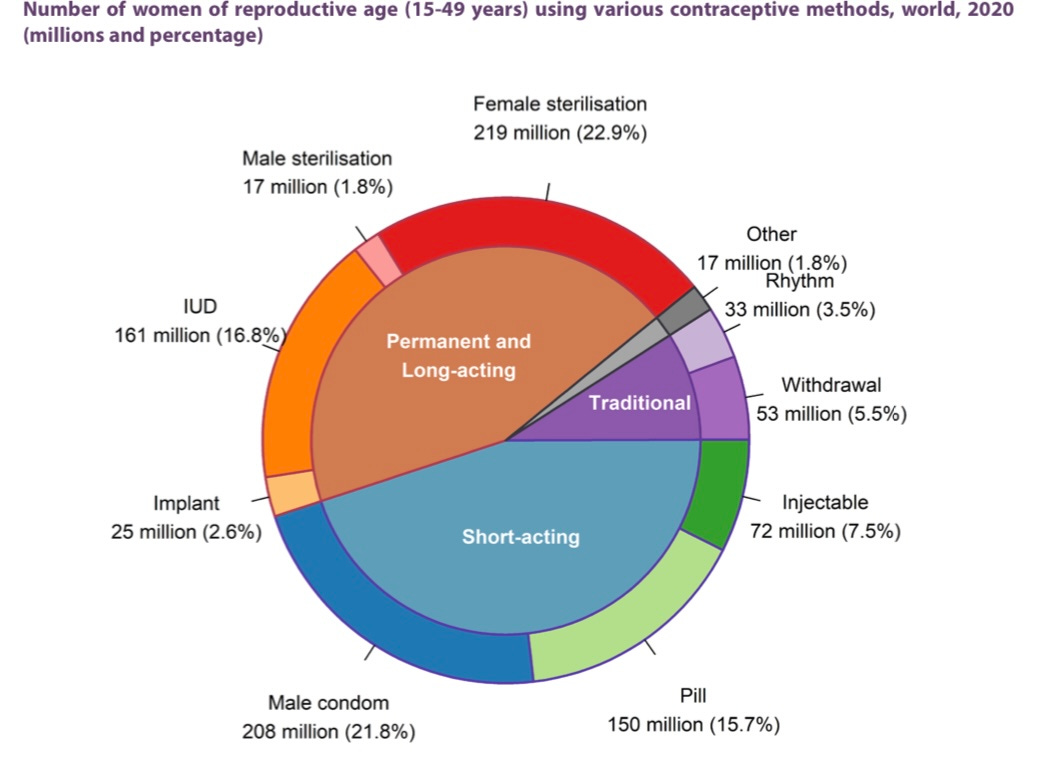
Vasectomy is popular in the country where I used to live. On the other hand, the United Nations pie chart shows fewer than 2% of men worldwide choose sterilization compared to 22% of women whose risks are not insignificant. Come on, guys, join the club! The disadvantages of sterilization are similar in the sexes, chiefly regret after a decision is made prematurely, and reversal by microsurgery is far from guaranteed. If the female tubes are completely removed by salpingectomy instead of tying them, the woman’s only option for conceiving is IVF. She does, however, benefit from a lower risk of ovarian cancer which often starts in the tubes. Not only dreadful, ovarian cancer is tragic when the organ is no longer needed, and it stole my mother’s life.
Time now to take a break for light relief.
A rejuvenation craze emerged in the badlands beyond the frontier of endocrinology a century ago. Clinics founded by maverick doctors offered testicular extracts as a tonic or grafts from cadavers and animals to boost vigor in older men. We are easily tempted to suspend disbelief in remedies that promise to conquer that universal villain, old age.
The famous Austrian physiologist Eugen Steinach would use none of those cures. He found another from research on rat testes. Sperm degenerating in their tubules after vasectomy created more space for Leydig cells to expand and increase testosterone output. From tying off one vas deferens he predicted health benefits without disrupting fertility. The Steinach operation soon became popular across Europe and America after men boasted about greater vitality and creativity. Among his celebrity patients, the Australian sexologist Norman Haire operated on the Irish poet W.B. Yeats at his Harley Street clinic. Yeats’ poems reveal an anxiety about aging and, besotted with Maud Gonne, he composed Broken Dreams as a lament at age 52.
…In the first loveliness of womanhood,
And with the fervour of my youthful eyes,
Has set me muttering like a fool.
You are more beautiful than any one …
Steinach was a fine scientist he blundered but this time. I almost regret the error because I might otherwise look forward to exceptional vitality in old age after being doubly Steinached!
You might suppose a couple of snips would never cause much trouble, except when coercive sterilization severs a precious right. Seven years ago a judge in Tennessee offered to reduce the sentences of offenders if they agreed to have vasectomy. Critics called it eugenic. A federal court reprimanded him and forced the practice to cease. That was but a minor squall compared to a hurricane that gave vasectomy a bad name in India.
Prime Minister Indira Gandhi announced a national Emergency in 1975, worried about national security, economics, and environmental decay. She had already come under pressure from Western countries to do something about population growth. And long after Margaret Sanger visited India, Paul Ehrlich stirred the public’s latent Malthusian anxiety with The Population Bomb. His opening chapter gives impressions of the crowded streets of New Delhi in 1968.
Government programs aimed to help the rural poor bullied men into mass vasectomy camps, offering a small plot of land or another reward in exchange. Over 6 million men underwent vasectomy in a year, many unwillingly while a few avoided pressure as the wealthy and well-connected generally do. Countless men suffered injuries or even died after botched operations. Having vasectomized dozens of animals I can only conclude the harm caused in a simple operation was from haste and carelessness. Gandhi’s Congress party was voted out of office the next year but its legacy lives on. As a sign of poor regard for the operation, out of 51 million sterilizations in India in the last decade, only 3% were vasectomies.
Western countries have nothing to crow about. The history of eugenic sterilization may sound remote but on a short drive from home, I could meet some of its last victims.
Harry Laughlin was the custodian of eugenics research records at the Cold Spring Harbor Laboratory in Long Island, New York (now a world center in molecular genetics). His 1922 book Eugenical Sterilization in the United States helped to shape state laws and became a copybook for Nazi eugenicists. Virginia’s Sterilization Act of 1924 gave this authorization for compulsory sterilization:
Be it enacted by the general assembly of Virginia, that whenever the superintendent shall be of opinion that it is for the best interests of the patients and of society that any inmate … should be sexually sterilized … for hereditary forms of insanity that are recurrent, idiocy, imbecility, feeblemindedness or epilepsy …
The superintendent of the Virginia State Colony in Lynchburg charged 18-year-old Carrie Buck as a genetic threat to society after the Act passed. He declared she inherited her mother’s feeblemindedness and promiscuity, blamed her for getting pregnant at age 17 after being raped by her foster parents’ nephew, and predicted her child would become another delinquent. The lawyer assigned to defend her in court acted half-heartedly from a conflict of interest as a former Colony board member. Carrie lost and again on appeal. The case passed to the U.S. Supreme Court presided over by former U.S. President William Taft, a zealous eugenicist. The Court concluded in Buck v. Bell (name of the Colony’s superintendent) that the Virginia law did not contravene the Constitution and it approved sterilization of the young woman against her will. Oliver Wendell Holmes, Jr., one of the most acclaimed jurists in U.S. history, avowed “three generations of imbeciles are enough.”
A later evaluation by a psychologist found Carrie had average intelligence. Her daughter’s name appeared on the school honor roll before dying of measles at age 8. Despite opposition to Buck v. Bell, half the states enacted statutes like Virginia’s. They led to over 60,000 involuntary sterilizations, many of them abuses of minorities that have since faded from the public’s conscience.
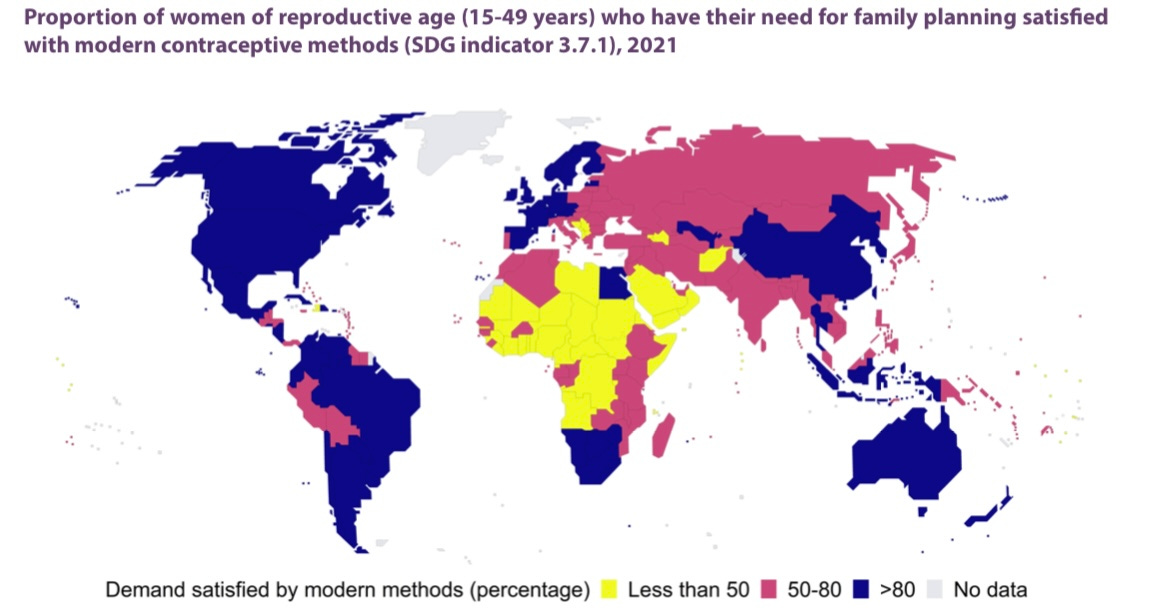
The escalating world population was never going to be relieved by forcing contraception or sterilization on people against modern sensibilities of reproductive rights and justice. However, population anxiety cresting in the 1970s led some of my generation to careers in reproduction research and education. We naively believed in technical solutions and underestimated the importance of social well-being and education for women, especially in the developing world. And yet, we weren’t completely wrong. Even today, more than half the 15 to 49-year-old population in most of Africa, Afghanistan, and (surprisingly) the Balkans rely on traditional methods of contraception. At home, we saw the Pill under fire for its high estrogen content and the detonation of the Dalkon Shield after medical and corporate scandals. Funding new methods became imperative for major funders, including the W.H.O., national governments, pharmaceutical companies, the Ford Foundation, and the Gates Foundation later on.
The watchword is non-hormonal. Not that hormones are entirely stripped of a role if they act on unique molecules at precise targets, ideally the egg and sperm. The problem with sex steroids and to a lesser extent progestins is they affect a thousand genes, making side effects inevitable.
Potential targets have emerged and submerged. I mention a few examples, including a couple of candidates for men. Monoclonal antibodies can stop sperm in their tracks, renewing hope for an immunocontraceptive. A search for a potent drug led to YCT529, an antagonist of a retinoic acid receptor that stops sperm production without causing hypovitaminosis A. It remains to be confirmed in human trials. Edinburgh researchers regarded the egg as their prime target. Antibodies blocked sperm from penetrating its thick membrane (zona pellucida) but closer study showed they also attacked the ovarian reserve. Translated to humans it implied premature menopause.
A veteran observer confided that investing in male and female condoms would have had a bigger impact on unplanned pregnancies than a grail search for the golden contraceptive arrow, and curbed the HIV-AIDS epidemic as a bonus. I am not that cynical, although I admit an irony. After commencing my career as a Population Council fellow I saw the pipelines for novel contraceptives drying up, so I followed my mentor to the filling wells of fertility treatment and fertility preservation after the birth of Louise Brown.
Promising contraceptives easily flop from failing rigid safety standards. We cannot allow any leeway for users who are young, healthy women and men compared to patients battling life-threatening maladies for whom drugs with trade-offs are acceptable. Family planning, a hard field to advance, is too important to let research slacken despite discouragement when paths halt in a swamp. Patient investment will eventually pay off, adding more options to the peculiar mix of contraceptives that have been around for aye. Success in research has its gloss and even prizes but, in closing, I wonder if it ever has as much impact as delivering a basic education in sexual physiology and reproductive health to people everywhere. I leave that question to better-qualified writers.
Illustrations: Reproduced under Creative Commons license CC BY 3.0 IGO from the United Nations Department of Economic and Social Affairs. World Family Planning 2022.
The next essay is a tribute to Jean Purdy, the hidden pioneer of IVF.
I remember a fertility conference in the late 1980s where one of the keynote presentations was about the need for more and better contraceptive choices to help control skyrocketing global population growth. His talk really made an impression on me, even though a lecture on contraception seemed to be out of place at a fertility conference! Some 35 years later, despite all the research, it seems the situation remains much the same. Your very interesting piece helps explain why - thank you.